
About

Adenomyosis occurs when the tissue that normally lines the uterus (endometrial tissue) grows into the muscular wall of the uterus. The displaced tissue continues to act normally — thickening, breaking down and bleeding — during each menstrual cycle. An enlarged uterus and painful, heavy periods can result.
Current Treatment Methods
Interventions for adenomyosis including hysterectomy, uterine artery embolization (UAE) and high intensity focused ultrasound (HIFU), hysteroscopic resection and radiofrequency thermal ablation (RFTA). Hysterectomy has long been offered as the definitive treatment for patients with abnormal uterine bleeding, dysmenorrhea, or bulk symptoms secondary to adenomyosis; Since the early 2000s, there has been a growing body of literature examining the effects of UAE in patients with adenomyosis who have completed childbearing; HIFU is a conservative nonsurgical treatment option adopted from the management of nongynecologic solid tumors, it has been reported successful and safe in patients with focal or diffuse adenomyosis; RFTA was first developed for use in solid tumors, such as osteomas and nonresectable liver tumors, and has been reported to be used to treat leiomyomata since 2002.
Chen J, Porter AE, Kho KA. Current and Future Surgical and Interventional Management Options for Adenomyosis. Semin Reprod Med. 2020 May;38(2-03):157-167. doi: 10.1055/s-0040-1718921. Epub 2020 Nov 5. PMID: 33152768.
What are the benefits of HIFU?
◼ It is non invasive, which means faster recovery comparing to surgery
◼ Only sedation, no anesthesia required
◼ Symptom relief of adenomyosis including improvement of dysmenorrheal and menstrual volume
◼ Significant reduction of uterine lesion volume
◼ Precisely ablate the lesion to preserve surrounding myometrium and endometrium and ensure less damage to the uterus
Am I suitable to undergo HIFU?
Suitable Indications:
◼ Patients present with dysmenorrhea and/or menorrhagia
◼ Diagnosis of adenomyosis confirmed by MRI
◼ Size of the adenomyotic lesion thicker than 3 cm
◼ Patients agree to undergo pre- and post-HIFU MRI
◼ Patients able to communicate with physician
*Please be noted the above criteria is only for reference, whether a patient can be applied HIFU shall be further confirmed by HIFU doctors after diagnosis.
Contraindications:
◼ Menstruating, pregnant or breast-feeding women
◼ Patients with suspected or confirmed uterine malignancy
◼ Patients with pelvic endometriosis
◼ Patients with abdominal surgical scar width>10 mm
◼ Patients with bowel adhesions to the uterus or the abdominal wall
Effectiveness of HIFU
Symptom Relief:
Many studies has evaluated clinical symptom after HIFU treatment and reported significant symptom alleviation. For example, a two-year follow-up study among 224 patients with adenomyosis treated by HIFU has shown that the clinical effectiveness of HIFU in alleviating dysmenorrhea in 203 patients who had completed the two-year follow-up reached 84.7%, 86.2%, and 82.3%, respectively at 3 months, 1 year, and 2 years after treatment; compared with the menstrual volume before treatment, the relief rates were 79.8% (87/109), 80.7% (88/109), and 78.9% (86/109) respectively at 3 months, 1 year, and 2 years after treatment.
In the other long-term study of total 208 treated patients, 173 (83.2%) achieved clinical success with varying degrees of alleviation of their symptom of dysmenorrhea. The VAS scores showed a considerable reduction from a baseline mean of 8.9 ± 1.4 to 3.4 ± 2.9, 3 months later (P < 0.001). The overall effectiveness rates were as follows: complete relief in 63 (30.3%); significant relief in 97 (46.6%); partial relief in 13 (6.3%). A total of 71% patients were asymptomatic during follow-up, of whom 19 patients had been menopausal. In addition, the hemoglobin increased to the normal level in 35 patients after treatment.
Fertility:
Because of the lack of scar tissue on the uterus wall, patients with adenomyosis who received HIFU can attempt to conceive much sooner than after surgical treatment. Moreover, the risk of uterine rupture during pregnancy or delivery is lower than following surgical treatment.
In recent years, many case studies has reported positive pregnancy outcome. For example, Zhou et al. recently completed a follow up of 68 HIFU-treated adenomyosis patients who wished to conceive. Of these 68 patients, 54 conceived at a median of 10 months (range: 1–31 months) post-HIFU, and 21 of them delivered healthy babies. No uterine rupture occurred during gestation or delivery.
1. Shui L, Mao S, Wu Q, Huang G, Wang J, Zhang R, Li K, He J, Zhang L. High-intensity focused ultrasound (HIFU) for adenomyosis: Two-year follow-up results. Ultrason Sonochem. 2015 Nov;27:677-681. doi: 10.1016/j.ultsonch.2015.05.024. Epub 2015 May 27. PMID: 26050604.
2. Liu X, Wang W, Wang Y, Wang Y, Li Q, Tang J. Clinical Predictors of Long-term Success in Ultrasound-guided High-intensity Focused Ultrasound Ablation Treatment for Adenomyosis: A Retrospective Study. Medicine (Baltimore). 2016 Jan;95(3):e2443. doi: 10.1097/MD.0000000000002443. PMID: 26817877; PMCID: PMC4998251.
3. Zhang L, Rao F, Setzen R. High intensity focused ultrasound for the treatment of adenomyosis: selection criteria, efficacy, safety and fertility. Acta Obstet Gynecol Scand. 2017 Jun;96(6):707-714. doi: 10.1111/aogs.13159. PMID: 28437003.
Safety of HIFU
Generally, the most common bothersome symptoms were lower abdominal pain, pain or discomfort in the treated region, vaginal discharge, and superficial skin burns.
In a systematic review of 9 articles and a total of 1813 patients, adverse effects reported of HIFU for adenomyosis are listed as below:

This systematic review revealed that the overall rates of severe adverse effects and complications after HIFU for the treatment of adenomyosis were low at 2.8%.
Marques ALS, Andres MP, Kho RM, Abrão MS. Is High-intensity Focused Ultrasound Effective for the Treatment of Adenomyosis? A Systematic Review and Meta-analysis. J Minim Invasive Gynecol. 2020 Feb;27(2):332-343. doi: 10.1016/j.jmig.2019.07.029. Epub 2019 Aug 1. PMID: 31377454.
Case Study
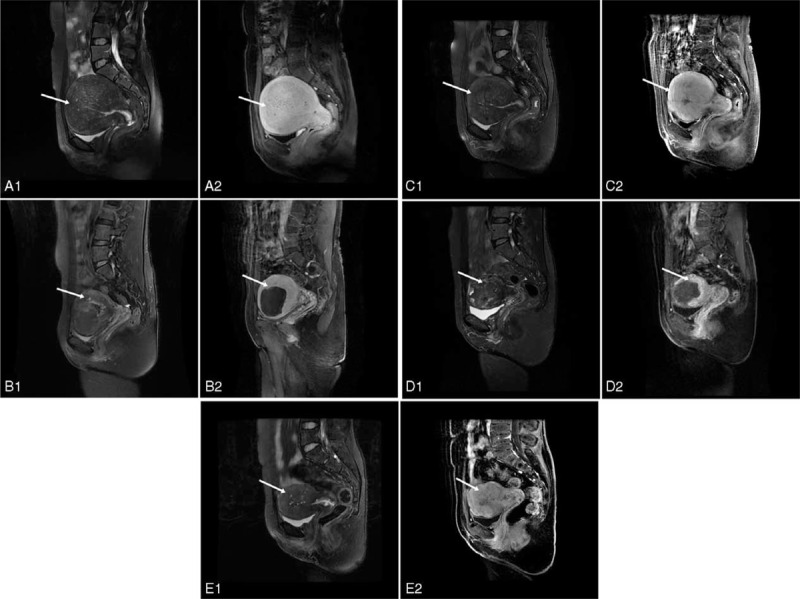
A 44-year-old woman who underwent twice USgHIFU ablation for symptomatic adenomyosis.
(A1-A2) Sagittal view of MR image obtained before the first USgHIFU ablation showed diffuse junctional zone thickening of the uterus (arrows). The volume of the uterus was 581 cm3.
(B1–B2) Sagittal view of MR image obtained 3 months after first USgHIFU ablation showed decreased size of the uterus. The volume of the uterus was 371 cm3. Arrows indicate non-perfusion area (183 cm3) after USgHIFU.
(C1–C2) Sagittal view of MR image obtained 48 months after first USgHIFU ablation (before second USgHIFU ablation) showed enhancement of the treated area (arrows). The volume of the uterus was 319 cm3.
(D1–D2) Sagittal view of MR image obtained 12 months after second USgHIFU ablation showed decreased size of the uterus. The volume of the uterus was 150 cm3. Arrows indicate the nonperfusion area (54 cm3) after treatment.
(E1–E2) Sagittal view of MR image obtained 24 months after second USgHIFU ablation showed enhancement of the treated area (arrows).
The volume of the uterus was 122 cm3. After twice USgHIFU, the patient was asymptomatic until she was menopausal. MR = magnetic resonance, USgHIFU = ultrasound-guided high-intensity focused ultrasound.
Liu X, Wang W, Wang Y, Wang Y, Li Q, Tang J. Clinical Predictors of Long-term Success in Ultrasound-guided High-intensity Focused Ultrasound Ablation Treatment for Adenomyosis: A Retrospective Study. Medicine (Baltimore). 2016 Jan;95(3):e2443. doi: 10.1097/MD.0000000000002443. PMID: 26817877; PMCID: PMC4998251.